
I’m currently doing some research on LASIK (Laser-Assisted In Situ Keratomileusis) surgeries, and this includes related procedures too.
I’d love to know from any readers who have done such surgeries, so please leave a comment below or contact me via email. I’d really appreciate your thoughts as I am considering having this procedure done myself.
The post serves as a handy place for me to record the research I’ve done so far.
There are millions of people who have been treated over the past 25 years or so that the technique has been in use to correct myopic vision (and similar conditions).
I’ve used lenses since I was 16 and by and large, am fine wearing them. The only major discomforts are the wintertime when it’s dry and windy, as my eyes feel dry very easily in those conditions. And of course, you’re always aware that your ability to function is wholly dependent on these delicate items you have in your eyes. I’ve never had any accidents with lenses, but still, the sense of dependence on them is not great. I know that without my lenses or glasses I would not be able to perform any of my daily activities, and I don’t like that feeling. From that perspective, surgery like Lasik would indeed be life-changing, and that is what I keep reading on forums and other outlets from people who had successful outcomes.
Now that I have kids, I also have much closer contact with them (hugging, playing etc) and glasses are a major nuisance in those situations. I also feel psychologically much better without glasses, but there are situations where they don’t perform as well as having good vision, for example while working at a computer.
Types of Refractive Laser Surgery
SMILE, LASIK, LASEK, and PRK are all refractive surgical procedures that use laser technology to correct vision problems such as nearsightedness, farsightedness, and astigmatism. Here’s a brief overview of each procedure:
- SMILE (Small Incision Lenticule Extraction): This is a minimally invasive procedure that uses a laser to create a small lenticule, or disc of corneal tissue, which is then removed through a small incision. The remaining cornea is reshaped, improving vision.
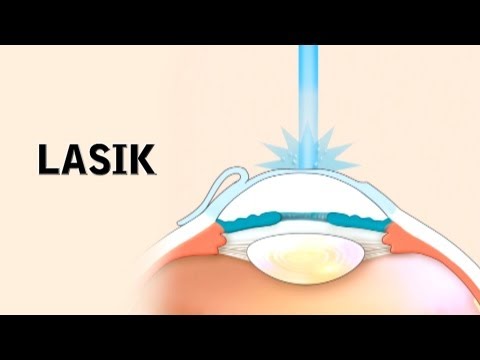
- LASIK (Laser-Assisted In Situ Keratomileusis): This is the most common refractive surgical procedure. During LASIK, a laser is used to create a corneal flap, which is then lifted to allow the underlying corneal tissue to be reshaped with the laser. The corneal flap is then repositioned over the reshaped tissue.
- LASEK (Laser-Assisted Subepithelial Keratectomy): Similar to LASIK, LASEK involves reshaping the cornea using a laser, but instead of creating a corneal flap, the top layer of the cornea, called the epithelium, is removed and then replaced after the laser treatment.
- PRK (Photorefractive Keratectomy): This is an older refractive surgical procedure that involves removing the top layer of the cornea and then reshaping the underlying corneal tissue with a laser. Unlike LASIK and LASEK, PRK does not involve the creation of a corneal flap.
Each procedure has its own advantages and disadvantages, and the best choice depends on the patient’s individual needs and anatomy.
SMILE vs LASIK
I asked above which technique suits me and never answered it, so here is where my reading landed. SMILE uses a much smaller incision than LASIK and creates no corneal flap, so fewer of the nerves that drive tear production get cut. The practical result is a lower rate of post-operative dry eye, which is exactly the side effect I am most wary of. It runs on the Zeiss VisuMax platform and has become a routine procedure rather than the novelty it was when I first looked into this. The catch is that SMILE has historically treated a narrower band of prescriptions than LASIK, and not every clinic offers it, so your exact numbers and local availability decide whether it is even an option for you.
The Lens Alternative: EVO ICL
Almost everything above is about reshaping the cornea with a laser. There is a second route I overlooked when I first wrote this: the EVO ICL, an implantable collamer lens that sits behind the iris and in front of your natural lens, like a permanent contact lens placed inside the eye. The cornea is left untouched, with nothing cut or removed.
For my situation this matters more than I expected. It doesn’t sever corneal nerves, so it doesn’t bring on the dry eye that bothers me every winter. It can be taken out again if my prescription drifts or something goes wrong, which a reshaped cornea cannot. And it corrects far stronger prescriptions than LASIK, up to around -15 to -20 diopters, because it never thins the cornea.
My -5 sits comfortably inside the range where either approach works, so for me ICL is not about needing it for the size of my myopia. It is about the dry eye and the reversibility. If you are dry-eye prone or carry a high prescription, put ICL on the table before committing to a laser. The trade-off is that it is surgery inside the eye, which carries its own small risks such as cataract, raised eye pressure, or the rare need to reposition the lens, so it is not a free lunch either.
One Lens for Both: EVO Viva
A standard ICL fixes only distance, so at my age it would still leave me reaching for readers before long, the same trap as laser. But STAAR also makes a version that gets around that: the EVO Viva, an extended-depth-of-focus ICL built to correct myopia and presbyopia at once. It has carried a European CE mark since 2020 and launched first in Spain, and it covers prescriptions well beyond my -5. Distance and near in a single implant, and still removable.
There is a catch, and it is the catch with every lens that promises vision at all distances. The extended focus is bought by spreading light, so you trade a little contrast and night-vision crispness for the near boost, and you get workable close vision rather than flawless reading of tiny print. Whether that trade is worth it turns on how presbyopic I already am. If my near sight is still fine, a plain ICL now with a near fix later may beat baking in the compromise today. That is a question for the surgeon, not a forum.
The Risks
While I’ve always heard that it is a fairly safe procedure, I also know that many optometrists and ophthalmologists don’t take undergo the surgery themselves, so I wanted to really dig a bit deeper to find out what the risks are and how many people are affected.
What I uncovered is that pretty much every country has its own associations of people who have come forward to share that they have had issues after undergoing the surgeries (see the one in Spain, or the one in the USA), some of them having quite horrific side effects, and some even being driven into depression and suicide. I feel deeply for people who have tried to improve their lives through surgery, only to bring on themselves a heap of misery. I’ve gone through similar experiences myself and I totally understand the despair and regret that can eat you from the inside in such situations.
The websites of such associations are a good place to start, however, they are not the best place to obtain a balanced opinion on the subject. Reading through such websites will inevitably leave you depressed and doubtful about the surgery. You can find such websites about many other types of surgeries, and I’ve even encountered several websites
Now I’ve seen many dubious clinics offering refractive surgeries, and with those, you’re really asking for trouble. They usually don’t have the latest machinery and you might get operated on by someone who has only been recently trained.
Sure, they might have a special offer in place, or just be significantly cheaper than other centers, but do you really wanted to be cheap when it’s your eyesight you’re gambling?
The lack of experience comes into play in the pre-operative consultancy phase. A good surgeon will be able to identify which patients he should operate and which don’t meet the pre-requisites for LASIK and should be directed to other methods of vision correction, or even dissuaded from doing any surgery. Unfortunately, some don’t have the experience needed to make these judgment calls, while others are just happy to operate on even those that are obvious 50/50 cases if it means pocketing a few more thousand euros.
So far, from my research, it definitely seems like this is a surgery that has risks, like any other surgery. These risks are compounded by the fact that the eyes are some of the most sensitive parts of the body, and are deemed absolutely essential to one’s quality of life.
I find it very believable when patients say that they have not been given full information before undergoing procedures. I’ve been to many doctors in my life and had my fair share of serious surgeries, and it’s a rare case when you find a doctor that really walks you through what they will actually to do to you, why, and also go through the possible side effects. The latter is the point most doctors ignore, in my opinion. Regulation is not always a good thing.
Yes, we can add more pages to a form explaining all the potential risks, but whenever I tried to read those consent forms, I always felt that things were overboard to the point that you just sign and hope for the best. That’s what happens when more emphasis is given to the legal side of things than common sense. The EU cookie policy comes to mind, as well as the terms and conditions of companies like Google and Facebook.
According to a 2009 study that the FDA conducted to understand the potential risks of severe problems that can result from LASIK, up to 46% of patients reported at least one visual symptom (like glare or blurred vision) at three months post-surgery. Up to 28% of patients reported dry eye symptoms, and less than 1% experienced “a lot of difficulty” with or inability to do usual activities because of side effects from their surgery.
There’s also a risk of infection after laser eye surgery. One recent study shows that this risk is somewhere between 1 in 15,000 and 1 in 30,000. The risk of infection from contact lenses, by comparison, is about 1 in 400. About 2% of people who undergo these procedures may require a second procedure.
On the other hand, according to the American Academy of Ophthalmology, 90% of LASIK patients see their vision improve to somewhere between 20/20 and 20/40.
The most vocal anti-LASIK doctor worldwide is Morris Waxler, although he ends up jeopardising his position through obvious conflict of interest, given that he runs a clinic aimed squarely at helping those who claim to have been injured by LASIK procedures. His claim to fame is that he was on the FDA committee that approved the procedure in 1996, and is now calling for it to be banned.
At the end of the day, like many other things in life, it’s a question of risk. If you’re happy wearing glasses and lenses, and have a small amount of myopia, I see no reason to risk it.
On the other hand, if your level of myopia is such that you are 100% dependent on having a pair of glasses around or using lenses, plus you have a problem wearing either of those and the condition is affecting your enjoyment of life (sport can be a pain with lenses or glasses, for example), then you are more than justified in seeking a solution like LASIK.
Lasik is generally a safe procedure, but like any surgery, there are some risks involved, including:
- Dry eyes: temporary or long-lasting dryness of the eyes, which can cause discomfort and visual problems.
- Glare, halos, and double vision: these visual symptoms can occur after lasik and affect nighttime vision.
- Corneal ectasia: this is a rare but serious condition in which the cornea bulges out and becomes thin after lasik.
- Regression: this occurs when the eye resumes its original shape, causing a loss of visual acuity and a need for additional surgical intervention.
- Starbursts around lights: this is a visual symptom in which lights appear as starbursts and can be caused by the laser reshaping of the cornea.
- Over or under correction: the laser may not remove enough or too much corneal tissue, leading to a need for additional surgical procedures.
- Flap complications: the corneal flap created during lasik can become dislodged, displaced or wrinkled, causing vision problems.
The FDA Revisits Informed Consent
When I wrote the original version I leaned on a 2009 FDA study for the numbers. There is now something more pointed. In July 2022 the FDA issued draft guidance recommending that every patient be handed a plain checklist of risks: dry eye, trouble driving at night, glare and halos, lasting visual symptoms; and that the surgeon go through it with them before the procedure. It followed years of patients saying they were never properly warned. That is the same complaint I made above about consent forms written for the lawyers instead of the patient, so it was good to see the regulator land in the same place. The guidance is still in draft, but if a surgeon already volunteers that checklist without being asked, read it as a good sign.
The Age Question: Will I Need Reading Glasses Anyway?
This is the objection I hear most often and understood least, so I want to write it out plainly. The claim is that fixing my myopia now buys me reading glasses later. Here is the mechanism. Around 45 the eye’s lens stiffens and loses its close-focus range, which is presbyopia, and it comes for everyone. A short-sighted person has a hidden perk here: take the glasses off, hold the page close, and you can still read unaided at any age, because the myopia itself works as built-in reading glasses. Make the eye emmetropic with surgery and you hand that perk back, so somewhere in your late forties you start needing readers for close work for the first time.
For me, at -5 and in glasses every waking hour, this is close to a non-issue. I would be swapping full-time correction for the odd pair of reading glasses, which is plainly an improvement. The argument really bites for low myopes who get by fine without glasses, or for anyone expecting to never touch a frame again and feeling cheated when readers turn up at 48. I am neither of those.
Two things here do deserve a real decision. The first is monovision, where the surgeon leaves one eye slightly short-sighted to keep your near vision; some people love it and others cannot stand the imbalance, and you can try it with contact lenses before committing to anything permanent. The second is the new wave of presbyopia eye drops, which are real but oversold as a cure. Pilocarpine drops like Vuity and Qlosi, along with newer formulas approved through 2025 and into 2026, shrink the pupil to create a pinhole effect that sharpens near vision for a few hours. They cost you some brightness, can bring on a brow-ache, have to be dosed every day, and carry a retinal caution worth raising with a doctor if you are myopic. Worth having in the toolkit, though not a reason to wave presbyopia away.
Why the Brochures Say 21 to 45
You see this age band everywhere, and it is a guideline rather than a wall. The lower end exists because your prescription has to stop moving before anyone cuts. Myopia often keeps creeping into the early twenties, and operating on an eye that is still changing just invites the correction to drift back. The upper end is presbyopia again, plus the slow march toward cataracts. Past the mid-forties, fixing distance with laser means readers soon after, and at that stage a lens-based route often makes more sense because it can take care of near vision too and head off the cataract you will probably get later. So the window is not the only safe time to do this. It is the stretch where reshaping the cornea gives the cleanest value, and at -5 I am near the far edge of it, which is exactly why the lens options keep pulling my attention.
Thinking in Lenses, Not Just Lasers
The more I read, the less this looks like a laser decision and the more it looks like a lens one. Three procedures sit in the same family, separated only by how far they go. An ICL adds an artificial lens in front of my natural one and can be taken out again. A refractive lens exchange swaps the natural lens out altogether for a synthetic one. Cataract surgery does the same swap, except age forces it once the natural lens clouds over.
That last one matters for the long view. Cataracts come for almost everyone who lives long enough, usually in the seventies or eighties, and the fix is to replace the clouded lens with an artificial one. Since the surgeon is choosing that lens anyway, they can set its power to correct your sight at the same time, and a multifocal or extended-focus version aims to give you distance and near together. Do that same operation early, before any cataract has formed, and it goes by the name refractive lens exchange.
Put plainly, if I plan to live a long life, my eyes are probably heading toward an artificial lens at some point no matter what I do now. That reframes the whole question for me. Reshaping my cornea today does nothing to change that destination, while the lens routes are already pointed at it. It is why a standard ICL, or the Viva, or eventually a lens exchange sits more comfortably with the long arc than carving the front of my eye.
Researching Clinics
If you’re in Barcelona, the top expert seems to be Dr. Jose Luis Guell, who is a co-founder of IMO, one of the best eye clinics in Barcelona.
The best clinics in Barcelona seem to be:
- IMO
- Quiron
- Clinica Baviera
In Malta, the best clinic is St James.
I’ve been to one of the more well-known clinics (not IMO) for a study that would determine whether I would be a candidate for Lasik or other similar surgeries. The equipment and clinic were top notch and I was treated very well, however, I got a distinct impression that this was a mass-production system, and I only got a few minutes with the doctor at the end of my two-hour session, where all he said was that I am a good candidate and there would be no problems.
This was followed by a lengthier session with the customer care lady who did the sales talk and assured me how safe it was, how life-changing, etc. I found this last part of the study to be the one that really put me off. I don’t want to discuss anything with a customer care person, I want the doctor to fully explain the risks and evaluate with me whether this is the right choice for my lifestyle and even current life conditions. I’d be ready to pay as much as needed for the doctor’s time, but sadly the whole system seems to be set up to very efficiently pass through a number of patients through the process every day with no further thought to it.
A friend of mine did the same study at another of the top clinics and came out with exactly the same impression.
What Actually Separates a Good Center
Since I first wrote the clinic notes above, I have come to think the procedure being routine is the least interesting thing about it. Millions are done well every year. What separates a good center is not the laser, which is much the same everywhere, but the screening, the readiness to turn you away, and the way it handles the rare complication. The best surgeon is the one most willing to tell you that you are not a candidate.
By that measure two names in Barcelona stand above the rest. Barraquer is one of the most respected eye hospitals in the world, a family institution running since 1941. And at IMO there is Dr. Jose Luis Guell, a past president of the ESCRS and a recognized authority on the ICL specifically, which is the route I am most drawn to. For me he is close to the ideal first consult, and Spain being an early market for the Viva lens means he has real experience with it.
What I had not appreciated is that the consult is the testing. A proper screening runs a couple of hours of measurements before the surgeon says a word: corneal mapping, thickness, dry-eye tests, pupil size in low light, and for the ICL its own set of readings such as the depth of the eye’s front chamber and a cell count on the cornea. The free studies the big chains offer cover the basics, but they are built to answer one question, whether you will buy the laser they sell, and the verdict tends to arrive from a salesperson rather than the surgeon. That was my experience at the well-known clinic above. The measurements were fine. What I objected to was the push to sign on the day.
My questions
- What technique is best suitable for me and why? What about the newer Smile technique vs Lasik?
- I have a big fear/reflex of anyone holding my eyes open and putting drops in, will this be a problem?
- Is there any test to determine whether I have dry eyes and whether this could be an issue that would make me not a good candidate for the operation?
- Which are the best machines for LASIK and does the center have them?
- What side effects or potential complications should I be wary of and when should I be worried about them?
- Will the treatment last forever?
Where I Have Landed, For Now
After all this I am still not booking anything, and that is a choice rather than dithering. The surgery carries a tail of follow-up visits in the weeks after, so it is not something to squeeze in around a busy stretch. The plan is to wait until the timing is right, then do it properly with a full screening at IMO where I can act on the result.
Waiting costs me almost nothing. My -5 is stable, the lens options do not expire, and the technology only improves in the gap. The one real price is the small year-on-year risk that comes with wearing contacts, so I am leaning on glasses a little more in the meantime. And the longevity angle settles it for me. I intend to live a long time, which makes me young for this rather than late, and a few years spent getting the procedure and the surgeon right is nothing against the decades of clear vision on the other side. Better to do it once, and do it well.
Additional Reading
- The FDA’s page on LASIK
- Informative video on LASIK – Dr. Jennifer Ling
- EyeWiki on LASIK complications – the American Academy of Ophthalmology’s peer-reviewed rundown, more balanced than the patient-advocacy sites.
Related





Leave a Reply